Anatomy of bone
Basic function of bone:
Bone is the basic unit of the skeletal system and provides shape and
support for the body, as well as protection for some organs.
There are 206 bones in human skeleton:
80 axial skeletal bones ( e.g. skull, vertebral column and sacrum)
120 appendicular skeletal bones (e.g. bones of extremities, scapula, pelvis)
Classification of bones:
Bones are divided on the basis of their location, shape, size and structure.
Based on location bones can be classified as follow:
- Axial skeleton – bones of the skull, scapula, vertebral column
Axial skeleton – bones of the skull, scapula, vertebral column
-Appendicular skeleton – bones of the pectoral girdle, pelvis and limbs
Based on shape bones can be classified as follow:
-Flat bone – bones of the skull, sternum, pelvis and ribs
-Tubular bone :
Long tubular bones – bone of the extremities (e.g. femur, humerus)
Short tubular bone – bones of the hands and feet
-Irregular bone – bones of the face and vertebrae
-Sesamoid bones – patella
Based on size bones can be classified as follow:
-Long bone – tubular bones of extremities (e.g. femur, humerus)
-Short bone – cuboidal in shape, in the foot (tarsal bones) and wrist (carpal bones)
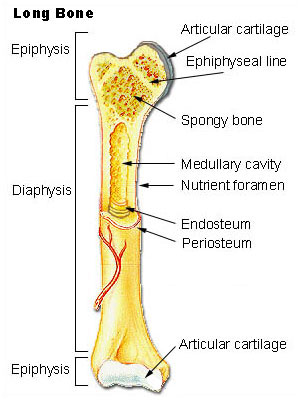
Gross structures of bones:
-Epiphysis – region between the growth plate or growth plate scar and the extended end of
bone, covered by articular cartilage.
-Metaphysis – region between the growth plate and diaphysis. Contains abundant trabecular
bone, but the cortical bone thins here comparing to diaphysis
-Diaphysis or shaft – region between metaphyses, composed mainly of compact cortical bone.
-Physis (epiphyseal plate, growth plate) – region of bone that separates the epiphysis from
metaphysic. Zone of endochondral ossification in actively growing bone or the epiphyseal scar
in a fully grown bone
Blood supply of bone:
The blood supply of bone varies with different types of bone, but vascular supply is especially rich in bones rich in red bone marrow.
Long bones blood supply:
-Diaphyseal nutrient artery – most important arterial supply. Pass obliquely through cortical
bone.
-Metaphyseal and epiphyseal arteries – numerous small arteries supply the ends of bones.These
blood vessels arise from arteries that supply adjacent joints, anastomoses with the diaphyseal
capillaries and ends up in bone marrow.
-Periosteal arterioles: these vessels supply the outer layers of cortical bone
Large irregular bones, short bones and flat bones:
- These bones are supplied by superficial periosteal arterioles.
Venous and Lymphatic drainage of bone:
- Blood is drained from the bone via venous and lymphatic vessels that accompany arteries and
frequently leaves through foramina near the articular end of bone.
Nerve supply of bone:
- Nerves are most rich in articular extremities of long bones, vertebrae and larger flat bones.
-Nerves accompany the blood vessels to the interior of the bone and to the perivascular spaces
of the haversian canals.
-The periosteal vnerves are the sensory nerves, which cause that periosteum is sensitive to
tearing or tension.
Bone tissue types and structure
Bone tissue can be classified based on texture, matrix arrangement, maturity and developmental origin.
Based on texture bone can be classified as follow:
-Compact bone (dense bone, cortical bone) – dense bone that surrounds trabecular bone in the
center. Contains Haversian system and secondary osteons.
-Sponge bone (trabecular bone, cancellous bone) – spongelike with numerous cavities. It is
located in the center of bone cavity and consists of conncted bony trabecules.
Based on matrix arrangement bone can be classified as follow:
-Lamellar bone – mature bone with collagen fibers arranged in lamellae. Lamellae of sponge bone
are arranged parallel to each other. In contrast lamellae of compact bone are organized
concentrically to around vascular canal (haversian canal)
-Woven bone – immature bone. Collagen fibers in woven bone are arranged in irregular random
arrays and contain smaller amounts of mineral substance and a higher proportion of osteocytes
to lamellar component. Woven bone is eventually converted to lamellar bone.
Histology:
Bone is composed of cells and a predominant collagenous extracellular matrix (type I collagen)
called osteoid which becomes mineralized by the deposition of calcium hydroxyapatite, which gives
the bone rigidity and strength
The cells of the bone:
Osteoblasts:
- Derived from primitive mesenchymal cells from multipotential bone marrow stromal cells of the
colony-forming unit of fibroblast lineage (CFU-F)
- Synthesize type I collagen, extracellular bone matrix, and noncollagenous proteins
- Line up along bone surfaces
-Characterized by round nucleus and abundant cytoplasm
-Control osteoblasts activity via parathyroid hormone (parathormone)
-Express parathormone receptors
Micro:
Positive stains: alkaline phosphatase, estrogen receptors, parathyroid receptors
EM: resemble fibroblasts due to well developed rough endoplasmic reticulum and Golgi
Osteoclasts:
- Derived from the hematopoietic stem cell-derived macrophage colony-stimulating factor
- Multinucleated motile cells randomly moving along the bone surface and eventually attach to
and resorb bone
-Osteoclasts acidifies extracellular area, which solubilizes the minerals and releases enzymes
which dissolves the matrix
-Produce resorption pits/bays (shallow concavities) called Howship’s lacunae
-Osteoclasts lack high affinity PTH receptors, which are on osteoblasts
-Major stimulator of osteoclasts activity is through its stimulation of osteoblasts PTH receptors
Osteocytes:
-Mature form of osteoblatsts embedded in the mineralized matrix
-Communicate with each other via osteocytic cell processes with gap junctions that travel
through canaliculi (bone tunnels)
-May maintain serum calcium and phosphorus level
Bone matrix:
Consist of organic and inorganic components:
-Organic component is composed of collagen fibers, predominantly collagen type I (95%) and
amorphous material, including glycosaminoglycans that are associated with proteins.
-Inorganic component represents about 50% of the dry weight of the bone and is composed of
abundant calcium and phosphorus and smaller an mounts of bicarbomnate, citrate, magnesium,
potassium and sodium.
Architecture of bone:
Haversian system (secondary osteomn):
- Primary structural unit of compact bone.
- It is a long often bifurcated, cylinder that is parallel to the long axis of bone.
-In the center of each haversian system is haversian canal, which is lined by endosteum and
contains a neurovascular bundle and loose connective tissue.
-The haversian canals connect with each other by transverse or oblique Volkman canals that
communicate with the marrow cavity and the periosteum to provide channels for the
neurovascular system.
Interstitila lamellae:
-Incomplete or fragmented osteons that are located between secondary osteons.
-Represent the remnant osteons left from partial resorption of old osteons during bone
remodeling.
-Mixture of of interstitial lamellae and osteons forms mosaic pattern.
-The age of the can be adjusted from the proportion of interstitial lamellae and intact ostreons.
Younger bone has more complete osteons than interstitial lamellae.
Circumferential lamellae:
- Circular lamellae that line the external surface of the cortex adjacent to the periosteum and line
the inner surface of the cortex next to the endosteum.
Histogenesis of the bone:
Bone tissue is formed by intramembranous ossification or byendochondral ossification. The original or model tissue is gradually destroyed and replaced with bone tissue. Woven bone is primarily formed
and later converted to lamellar bone by subsequent remodeling.
Intramembranous ossification:
-Source of flat and less commonly short bones
-Condensation of mesenchymal tissue
-Process begins when multiple group of cells differentiate into osteoblasts in a primary
ossification center
-Osteoid is synthesized and than mineralized surrounding the osteoblast which maturates to
ostecyte
-When ossification centers fuse, formation of loose trabecular structures known as primary
spongiosa is taking place.
- Subsequently blood vessels grow into the connective tissue between trabeculae.
Endochondral ossification:
-Responsible for formation of long and short bones.
-Hyaline cartilage model which provides template of the shape of the bone
-May be divided into 2 phases:
1st phase chondrocytes are hypertrophic and degenerated, and then calcified
2nd phase osteoprogenitor cells and blood capillaries invade the spaces left by degenerating cartilage (osteoblasts arise from osteoprogenitor cells and lay down a layer of rapidly mineralized osteoid on the surface of calcified cartilage, and is forming primary spongiosa, which later is remodeled to lamellar bone (secondary spongiosa). Calcified cartilage is resorbed by chondroblasts and replaced by bone and marrow cavities.
Epiphyseal cartilage of long bone is located between epiphysis and metaphysic and is responsible for longitudinal growth of the bone
Epiphyseal cartilage has 5 zones
Resting zone - small chondrocytes
Proliferative zone – rapidly dividing chondrocytes in columns, parallel to the long axis of bone
Hypertrophic zone – large chondrocytes with clear cytoplasmic glycogen,
Calcified cartilage zone (zone of provisional calcification) – chondrocyte graveyard, followed by blood vessel invasion and bone deposition
Ossification zone – formation of primary spongiosa by rapidly mineralized osteoid
Growth of the bone:
-Bone grows by either endochondral or intramembranous ossifications.
-Endochondreal ossification of the epiphyseal plate is responsible for longitudinal growth of the
long bones.
-Periosteal deposition is responsible for both the length and thickness of long bones
-Endosteal bone deposition is responsible for growth of trabecular bone and the endosteal cortex,
including the haversian system.
-Bone formation is an ongoing process that alters the size and shape of bone by partial resorption
of preformed bone tissue and simultaneous deposition of new bone (modeling and remodeling)
Modeling is a process in which bone achieve its proper shape.
-Modeling is responsible for the circumferential growth of the bone and expansion of the marrow
cavity.
-Remodeling is a continuous process, in which damaged bone is repaired, ion homeostasis is
maintained, and bone is reinforced for increased stress.
-In adults, the remodeling rate varies in different types of bones.
-Trabecular bone is remodeled at a higher rate (25% per year) than that of cortical bone
(3% per year) in a healthy adult.
-Resorption and deposition are normally balanced, and bone density is maintained.
Resorptive activity exceeding deposition activity in a pathologic state may cause lytic lesion.
-The cement line (reversal line) is evidence of previous remodeling activity and is formed by filling
of new bone in a previously resorbed cavity.
- The cement line is strongly basophilic due to the high content of inorganic matrix and is
normally found in the haversian and interstitial systems of adult bone.
-Amount of cement lines corresponds to the activity of remodeling that has occurred
(entire remodeling cycle requires approximately 6 months)
-Cement line that results from normal remodeling is relatively long and straight, an indented or
mosaic pattern indicates a pathologically accelerated remodeling process.